RSI Article: RSI News of 03/16/2024
Archive
Today (September 8, 2024) I will begin to describe the strange events that happened to me in the days following my awakening.
Even today, I cannot define whether they were dreams or hallucinations. Was I sleeping? I do not think so; the images, the details, and the smells were so real that they lead me to believe they were hallucinations, but I cannot be certain. They were so absurd as to be at the very least incredible, yet extremely rich in detail.
They were so real and intense that I lived them, and they are now part of my history and my experience of that period.
The first “hallucination-dream”:
I was in my bed in intensive care at Cardiocentro Ticino and, to pass the time, I was browsing the internet on my computer. This was impossible, as at that time I was completely paralyzed and could move neither my arms nor my legs… anyway, let us continue.
One day, on a specialized canine website, I saw a new variant of my dog: a Labrador with webbed paws that was very effective and high-performing in all aquatic disciplines.
This is an image constructed with artificial intelligence based on my memories:

I had to have it!
I wanted to find a special dog that could keep my Kila company.
In this case, the image represented is real:

This strange puppy was in Benidorm, Spain. It was a Labrador selected for swimming in the sea, capable of diving to great depths without any problem.
The problem was how to leave the hospital and how to get to Spain in my condition.
One day I spoke about it to Dr. Paul (see chapter Doctor Paul); I explained the peculiarities and the rarity of this puppy, as it was the first litter with these characteristics.
Dr. Paul saw my enthusiasm and at that moment said to me: “I will take care of it. I will see how to organize things, and as soon as I have two days off, we will go.”
To myself, I thought, “Sure, okay, but how does he plan to get there?”
After a few days—I do not remember how many—at around six in the morning, I saw Paul arrive. He was not wearing his usual green scrub top and trousers, nor was he wearing the usual green plastic clogs he wore; he was in jeans with a very colorful Hawaiian shirt.
He approached my bed, leaned toward me, and whispered: “We are leaving; put your arms around my neck.”
I had not noticed that there was a wheelchair next to Paul; as soon as I saw it, I immediately clung to his neck. Paul lifted me and then gently placed me in the chair.
We slipped out quietly, avoiding being seen by the hospital staff; to exit, we used the access that Rega uses to deliver its patients.
First success: we were outside. It was a spring day, not too cold, with a very pleasant breeze.
But how would the journey to Spain continue now? By what means? A van, by car?
Paul was pushing me, but I knew nothing; I did not know where we were going.
At a certain point, I saw that he was heading toward the motorcycle parking lot of the Ospedale Civico.
I was surprised and worried. I could move neither my legs nor my arms; how could I get onto a motorcycle? Even though motorcycles have always been my passion—in fact, before my illness, I had just purchased a splendid, fully equipped 1200 cc Triumph Tiger—I would never have been able to get on it, let alone hold on to avoid falling.
Paul stopped in front of a huge Harley Davidson, complete with a top box with armrests.
He lifted me from the wheelchair and placed me on the rear seat of the motorcycle and, while holding me, secured me to the top box with a strap. He put the helmet on me, got on the bike, and we set off.
To myself, I said: “Nice, but going to Spain by motorcycle is really long; by the time we arrive, I will be dead!”
But no, he did not head toward the highway, but rather toward Bioggio and then Agno.
We arrived at Agno airport and entered through a service gate at the end of the runway; from there, he headed toward the hangars. He entered one of them and parked the motorcycle next to a small propeller plane.
The idea was excellent, but where was the pilot?
In the hangar, there was only him and me; even outside, not a living soul was to be seen.
He unstrapped me from the motorcycle and, using the same technique as before, I clung to his neck so that he could lift me and carry me inside that small four-seater propeller plane.
The hardest part was climbing the stairs with me clinging to his neck and entering through that narrow, cramped door, but after a few failed attempts, we succeeded.
He placed me on the seat and fastened my seatbelts; now we just had to wait for the pilot.
But no, Paul sat in the front in one of the pilot seats, fastened his seatbelts, put on his headset, and began to tinker with buttons and levers.
At a certain point, the first engine started, and shortly after, the second one did too; soon after, the plane began to move and we left the hangar.
I was truly worried, as I did not know if Paul was capable of piloting a plane, let alone if he had a license.
I gathered my strength and whispered to him: “Paul, do you know how to fly?” At that time, I still had a tracheostomy, so I could not speak unless the speaking valve was fitted, and in that case, I did not have it.
In any case, Paul saw my concern and, reading my lips, understood what I had said to him.
He replied that he did not have any valid license, but that he had learned to fly in the Netherlands during his military service. Yes, Paul was Dutch, but he had lived in Switzerland for years and worked at Cardiocentro Ticino as an intensive care nurse.
To be continued… I will take a short break now.
During the first few days after my “awakening,” I constantly heard the name of a certain Dr. Paul; he resolved all complications and unforeseen events.
Both doctors and nurses turned to him in case of doubt, and as soon as an emergency arose, he was the first to be called.
In short, more than a doctor, he was a kind of superhero; he was always present, and if he wasn’t, he would arrive within a very short time (seconds).
Reality or hallucination? To be precise, I still do not understand it even now; it seemed so real that it is difficult to consider it a hallucination.
Perhaps a mix of the two?
A few days after I woke up, my wife came to visit me and on that occasion she asked: “Don’t you recognize him?”
Personally, I didn’t feel like I had ever seen him; furthermore, with the mask on, it was difficult to recognize people.
Keep in mind that during that period I was pumped full of drugs, I still had the tracheostomy and the nasogastric tube, as well as venous and arterial devices entering through my arms and neck, and to top it all off, I also had a urinary catheter.
Being dazed and having hallucinations could be considered a “normal” condition.
In any case, I shook my head “no.” And she said: “But it’s Paul, our friend, don’t you remember?”
I was surprised; I knew Paul worked in the hospital, but I didn’t remember him being a doctor.
Well, yes, I had convinced myself that Paul was the Super Doctor who solved all the problems for us patients.
Instead, Paul is a dear friend of mine whom I already knew before my illness.
He is an intensive care nurse with vast experience (perhaps that is why I saw him as Doctor Paul) whom I came to appreciate as a person and as a professional during and after my hospitalization at Cardiocentro Ticino.
During my hallucinations, he was always with me, getting me out of trouble and helping me resolve the various dangerous situations I got myself into, but I will tell you more about that later.
He was one of the nurses assisting me, but not knowing my habits, he would shave me completely while I was sedated.
Yes, because I have always kept an “unshaven” beard, whereas he loved “clean,” hairless faces.
Paul is one of those “old school” nurses with incredible experience, who is always on the move (day and night) and always in contact with his patients; he continues to go from bay to bay, interpreting the patients’ status from small signs like skin color, eyelid movements, drops of sweat on the forehead… in addition to the various instruments provided in intensive care units.
A few months after my discharge from the hospital—a discharge that was… forced at my request—I invited him, his wife, and our mutual friends Maria Antonietta and Alexander to lunch.
Alexander is a real doctor, and not the fruit of my imagination.
The discharge was forced because I no longer wanted to be away from home, away from my wife, my children, and what remained of my family; yes, the loss of my parents was giving me a sense of emptiness that I could not fill.
On that splendid summer evening, thanks to my wife and the delicacies brought by Maria Antonietta and Paul’s wife, we were able to spend a wonderful evening together.
On that occasion, Paul gave me a book, in English, titled “BREATHE IN BREATHE OUT, A Surviving ECMO Story.”


At first, that gift had unsettled me, partly because of the language and secondly because of the subject matter; I had lived that experience, it had not been pleasant, and the results were not what I had expected!
Yes, I had survived, but at what price and with what damage.
For the first few days after the dinner, I left the book in a corner and ignored it.
After a few weeks, I began to leaf through it, but my English is limited; I had to use my phone’s camera to photograph the pages and then translate them with software. It became very laborious!
For a while, I gave up, but the content of that book intrigued me; I wanted to know if someone else had gone through my experience, if they had gone through what I had gone through.
However, my English did not allow me to read it.
I tried to find an Italian copy, but the book has not been translated into other languages.
I tried to find a digital copy to feed into translation software, but that option was not feasible either.
I was curious to know how Adam York had faced that terrible experience, even though it wasn’t about Covid—it was in 2018, so before the pandemic.
Recently, in mid-November 2023, I made up my mind; I had the book cut at a stationer’s so that I could digitize the content using a scanner.
Now I am translating the entire book, one chapter a day, using translation software and then revising the translation from a literary perspective into Italian.
It is a lot of work, but it allows me to read the book more deeply and to grasp the feelings that Adam wanted to convey with his writing.
And why not… maybe I could ask the author if he is interested in having his book translated into Italian.
To be continued….
This book, the suggestion from Carmen (Paul’s colleague), and the meeting with the post-intensive care self-help group at Cardiocentro Ticino convinced and motivated me to create this blog and, in the future, perhaps even a book and/or a documentary video.

The Exercise Bike
I had been “awake” for a few days (according to the medical diary, around March 7, 2021) and the doctors had decided that I needed to begin restoring the musculature that had wasted away over the previous months.
In the morning, a very young and athletic man would arrive; he would take my limbs and move them passively, as I did not have the strength to move anything except my hand.
During that period, I was also worried because I had no sensation in my lower limbs or my right arm; this frightened me greatly and made my state of mind very dark and pessimistic.
One afternoon, however, he arrived with a mini exercise bike and placed it on the bed.
I felt like laughing, if not crying—how was I supposed to pedal if I couldn’t even feel my legs?
He took my legs and fastened my feet to the pedals with Velcro, then turned on the machine and suddenly I was pedaling… or rather, the machine was making me pedal without me doing practically anything.
However, it was another milestone I had reached; they were all very small milestones, and this condition made me impatient and demoralized for not being able to do more. I was accustomed to more concrete goals, and these seemed “useless” or almost so. But gradually, as everyone kept telling me, some improvement began to show, even very small ones; one milestone I was missing was being able to eat independently and not with that feeding tube.
Going Outdoors with Carmen
By now, I was able to sit in an armchair for hours.
I spent my time observing what the nurses were doing, aware that as a former professional rescuer, my knowledge made me very critical in judging various medical procedures, the order of actions, and the methods used.
After a few days, however, the routine began to grow tedious and time dragged on.
One morning, to my great surprise, a nurse named Carmen arrived and suggested I go outside for some fresh air. At first, I was frightened; moving from intensive care to the outdoors was by no means a given, and I had never heard of a procedure or therapy that included such an action.
To be honest, I was fearful; in intensive care, I was controlled and monitored, I had a ventilator at hand and everything that could keep me alive in case of an emergency, but if something happened to me not just outside of intensive care, but outside the hospital entirely, what would happen?
Carmen immediately calmed and reassured me; she had an oximeter at hand—or rather, at her fingertip—and we would also bring an oxygen tank with us. I was afraid, but I couldn’t wait to get my nose outside and feel the freshness and temperature of the outdoor air, and perhaps catch a scent.
Once I was in the armchair, she wrapped my body in a blanket, so that practically only my head was visible. She took me outside in front of the hospital helipad; no helicopter arrived, but instead, there was a constant flow of people entering and leaving through that door. Some went out to smoke and others entered to go to work; I was no longer used to seeing so many people and it exhausted me, even though I didn’t have to interact with them. It was one of the most beautiful experiences I had during my hospitalization, even if the only scent I managed to catch was that of cigarette smoke. Two other exhilarating experiences were the first glass of water and the first lemon gelato, but I will tell you about those another time.
Eating and Drinking: A Spontaneous Action
Bringing food to the mouth, chewing, tasting, swallowing, digesting… and finally evacuating; these are all actions taken for granted, physiological. Unfortunately, during these months, my body had forgotten all these automatic processes.
Even though the doctors had decided not to reinsert the nasogastric tube after I had pulled it out, I was not allowed to eat or drink anything; I had to wait for an evaluation by the speech therapist before I could consume anything at all.
I thought it would be natural to be able to return to nourishing myself, but I soon had to change my mind.
The speech therapist arrived, a young woman with long blonde hair; she vaguely reminded me of my daughter, Asia.
She had a tray with some purées, water, and a bluish liquid.
She introduced herself and told me she had come to evaluate whether I was capable of swallowing solid or liquid foods.
I was fairly calm, even though I still had the tracheostomy; without the nasogastric tube, I felt better and—mistakenly—I thought to myself: how hard can a swallowing test be?
She had me open my mouth and placed some drops of this blue liquid on my tongue.
Afterward, she gave me a few teaspoons of water and had me swallow them, then told me to cough; it seemed to me that the test had gone well. She asked me to open my mouth and show her my tongue, which I did; convinced I had passed the test, I opened my mouth wide.
She looked at my oral cavity and immediately said, “Unfortunately, we must stop here; you have dysphagia, and if you were to ingest liquids or solids, they would very likely end up in your trachea and lungs.”
I was discouraged; I had been convinced that I had passed the exam without problems and that I would be able to eat a few hours later.
In the following days, they gave me only liquids with a thickener that turned the water into a kind of jelly, disgusting in both taste and consistency.
Every day I asked to repeat the test, but the speech therapist was unavailable, or perhaps they told me that because they felt it was too soon to repeat it.
Finally, after a week of jelly, I was able to repeat the test. I was nervous and tried to concentrate on swallowing and coughing in the best possible way so as not to have that blue liquid in my mouth anymore.
With a smile, she told me I could start eating a dysphagia diet; in practice, all foods were blended and turned into a purée. Inviting? Not in the least, but better than nothing.
When the speech therapist left, I immediately asked for a glass of cold water; they brought it to me after a few minutes.
The nurse stayed nearby to ensure I had no problems swallowing the water.
I took the glass and began to sip a drop; it was better than the finest Champagne I had ever tasted. I hadn’t had a drink of water in three months.
That glass of water gave me an exhilarating sensation, and in that moment, I felt fully satisfied and fulfilled. The food, on the other hand, was not the best; those blends of meat and vegetables mixed together were not inviting either visually or in terms of taste; I couldn’t tell what I was eating.
At the end of the meal, however, came the second greatest satisfaction: a lemon sorbet, a true delight.
The coolness of the ice cream going down my throat and the citrusy taste of the lemon, so refreshing, left a good flavor in my mouth. Water and lemon sorbet were the two things that provided the best sensations—sensations I hadn’t felt for a long time.
The nurses had stocked up on lemon sorbet to make sure I didn’t run out, as vanilla and chocolate ice cream did not give me the same sense of pleasure.
I had been in intensive care for many months and by then everyone knew me; they all pampered me and tried to make my stay as pleasant as possible, even though the cannulas and devices invading my body were still many and I didn’t know when they would be removed.
Day after day, I managed to reach a small milestone and obtain small satisfactions; the road ahead was still long and I often fell into frustration and discouragement, but then I would get back up and try to face the next obstacle.
ETHZ Article: “Therapeutic Success Thanks to Determination and Robots”
After suffering from a severe case of Covid-19, Roger Gassert discovered firsthand how important rehabilitation is for recovery.
The ETH professor of rehabilitation engineering now intends to ensure that patients benefit from his developments.
https://ethz.ch/en/news-and-events/eth-news/news/2023/12/globe-portraite-roger-gassert.html
Time passes and some memories resurface
October 31, 2023: yesterday I had the flu vaccine, and on 10.11.2023 at 10:00 AM, I will receive my sixth Covid vaccine.
I do not know how it will be, but up until the fifth, I always received the full dose (not the booster) of the Moderna vaccine.
Today I feel as if I have been hit by a semi-truck.
It is 12:40 AM and I cannot sleep; lying down, I struggle to breathe. I raise the head of the bed and sit up; it has not solved the problem, but it is better.
The cough is testing my physical body, but not my mind; they are two individuals traveling at distinct paces from one another.
With every breath, my chest hurts; it feels as if the air has to travel a much longer distance to reach my lungs. In that stretch, the little air I inhale disperses somewhere or perhaps is absorbed by something else, but not by my meager lungs.
My mind, however, is afraid; it thinks about everything I have been through, about the Advance Directives in case I lose the capacity for discernment and am unable to express my will—a document I have drafted and left with my wife and her cousin (and of which I am certain).
But if something happens to me suddenly, what do I do?
I am not afraid of dying, but I am terrified of suffering, of going through that experience again, of having that hunger for air again that my body could not satisfy.
My mind races, and during those thoughts, the first few months after sedation came back to me.
In those days, it felt as if I were wearing a garment that did not belong to me.
My body was no longer mine; it was an entity that had traveled a long and disastrous journey without me.
It was no longer my physique; I did not know, I did not remember, and I had not experienced what my body, instead, was showing me and wanted me to see.
A harsh and at times fatal path that had tested it more than once, a wandering that had drained it of all the energy it possessed. It had been left abandoned and defenseless, without energy, without the strength to perform simple actions such as moving a finger or a muscle; no sound would emerge from its vocal cords anymore.
It no longer had the will to live or to fight; it had been forced to do so for too long and too many times. It was time to rest and recover the energy it had been required to expend in all those challenges for survival.
This, I did not know.
I remembered a functioning body that had given me much satisfaction and that I could and had tested multiple times without any problem; it had never disappointed me and had never rejected my orders.
I did not know him, he did not understand me, and I did not understand him; we were two strangers placed there, side by side, without even having been introduced.
Yet both had to fight a hard and difficult battle, a battle that had to be fought alongside each other and not against each other.
Instead, he seemed to be fighting against me; I did not know that this stranger had already had to fight many battles alone before allying with me.
I did not know him and he did not speak to me, he told me nothing about himself; we were two strangers placed there by someone with a power beyond our will and without any regard for our safety.
What would the future be with this broken-down companion with little energy to spend?
I do not know; nearly three years have passed, but I still do not have an answer to this question.
It is better now; the breathing is more relaxed, each breath is longer and deeper.
It is time to rest not only the body but also the mind!
Sleep, it is 2:23 AM!
Yes, but in this chapter, I wanted to tell you about my memories during the period spent in intensive care at Cardiocentro Ticino.
To be honest, I do not have many memories; I recall moments of lucidity to which, however, I cannot assign a chronological order.
Today is January 17, 2024; three years ago at this time, I was in the middle of this adventure. As you may have read, in those days I had been transferred to the intensive care unit of the Moncucco Clinic.
Let us return to my awakening after my body had to overcome all the various challenges to become an entity devoid of energy and functionality; it was a body placed there, lying in a bed, inert and immobile.
The Awakening
In the first days after awakening, my wife came to visit me; my eyes were half-closed, I was lifeless, I absorbed her words passively, without any interest.
On one hand, it was pleasant; I felt dissociated from reality and worries. Nothing interested me; I was at the mercy of my fate in a passive way. I did not have the strength to move a finger, let alone react to what was happening to me.
On that occasion, my wife Mirna said to me: “As soon as you are better, we will go on vacation to a magnificent place.”
I dreamed of a Caribbean sea, where I had never been, a postcard-perfect sea.
My dream was and is French Polynesia, the island of Taha’a (I fell in love with it after seeing it in a documentary).
Unfortunately, however, my physique had returned to that of a “child.”
A one-year-old child begins to walk; I did not!
A one-year-old child begins to eat independently; I did not!
A one-year-old child begins to speak; I did not!
A one-year-old child learns to grasp objects; I did not!
I could not speak because I had a tracheostomy, but even if I could, my body did not have the energy to do so and my mind did not feel the need.
I could not move, shift, or simply turn over in bed.
I did not have the strength to lift my arms; I could move the fingers of my left hand, but they were trembling. The weakness… and also my morale made everything difficult, impossible.
The X-ray machine
Almost every day, generally in the morning, I heard the sound of an electric motor; it was the machine they used to take X-rays of my lungs.
I did not have to do anything, also because I could not.
They would move me, “photograph” me, and then leave with their motorized device.
I remember that one day the device did not work as it should; it was out of battery, and the technician was cursing at whoever had used it before him and had not put it on charge.
This noise was a “routine” that allowed me to orient my mind within the day.
I often waited for it impatiently to understand if it was morning or afternoon; evening, on the other hand, I could recognize by the absence of light outside the window and the lights in the room. It had become my “biological clock.”
The tracheostomy
During the period when I had the tracheostomy, no sound came from my mouth, although in some cases my wife read my lips and managed to understand a few words.
Several months after I returned home, she told me that the first time she came to visit me, I shouted at her voicelessly, “Call a taxi and take me home.”
I remember nothing of that day, nor of that visit.
I recall that I communicated with gestures using my left hand; I would point my index finger toward my throat to indicate to the nurses that I wanted to be suctioned through the tracheostomy.
Periodically, several times a day, I had to do this because phlegm would settle and make breathing difficult for me.
They would insert a small tube into the tracheostomy hole and go down to suction the various fluids that had settled.
There were nurses who were more hesitant or perhaps had less experience who limited themselves to suctioning “on the surface”; in those cases, I did not feel much improvement. But when they suctioned deep down, I felt as if I were coming back to life and afterwards I felt more relaxed.
It was not pleasant, but it was certainly better than when the tracheostomy became clogged and I had to strain to get air into those lungs battered by Covid.
After a few days… or perhaps weeks, during one of my wife’s visits, one of the nurses—I don’t remember who—said: “Let’s try putting on the speaking valve so you can have a chat with your wife.”
My wife and I looked at each other in amazement.
I immediately signaled “OK”; finally, I would be able to communicate.
My wife was a bit frightened by this unexpected and sudden proposal; she said to the nurse: “But does the doctor know?”
Reassuring her, the nurse told her that there would be no danger and that he would be just a few meters away.
They connected this valve to my tracheostomy and, as if by magic, I heard my voice, even if it was not my usual voice.
Perhaps the valve, or perhaps my energy levels, did not allow the sound of my voice to come out as it did before the illness, but regardless, I was able to speak, to communicate, to express myself… it was one of my first successes!
It lasted only a few minutes; speaking exhausted me very quickly, as if I were chopping wood or lifting bags of cement, but that is how it was: a few words and I was exhausted, feeling the need to rest and sleep.
So I did; I said goodbye to my wife, closed my eyes, and went to sleep, happy and satisfied to have overcome my first challenge.
The nasogastric tube
I do not know exactly when, but one day, while washing my face, Paul accidentally pulled out my nasogastric tube. I hardly noticed, and I was pleased—maybe I could start tasting something by mouth.
Instead, after a few minutes, he returned with a bag and various materials; he told me that he would have to put it back in because I was not ready to eat.
Now I was conscious, and inserting that cannula from the nose down to the esophagus caused me incredible pain; I can still feel the burning and the obstacles the tube encountered on its path to its destination.
Paul, with his Dutch accent, told me “swallow so it goes down better,” but the tube struggled to go down… not to be repeated.
From 그 moment on, every time someone approached my face, I was terrified they might remove that cursed tube.
That tube was used to feed me; I remember the bags that were connected and the strange aftertaste that rose from my stomach, a taste that was not pleasant at all.
Some medications were also administered via the nasogastric route, in particular the therapy against leukemia.
I remember a small electric grinder in which they placed the medications, grinding them until they became a powder that they dissolved in a liquid; they would draw it up with a huge syringe and then inject everything through my nose.
The pleasant part was when they injected Coca-Cola to “flush” the tube after administering the medications; in that moment, I felt a pleasant sensation. To be clear, I did not taste it, but I could perceive the freshness of something going down through my throat and into my stomach.
After a few days, while trying to blow my nose, I pulled out the nasogastric tube myself. It was exhausting to reach my nose with my trembling left hand, and the tremor caused me to yank the tube out. I could not use my right hand; my dominant hand was not moving.
I was desperate; I did not want to go through that ordeal once more, but I could not express it except through tears and a few signs with the fingers of my left hand.
Fortunately, the nurses noticed and spoke with the doctor to determine if it was necessary to reposition the cannula or not.
Fortunately, they did not put it back; it meant starting to eat and drink.
I was overjoyed.
But my enthusiasm was soon dampened; before eating, I had to have the consent of the speech therapist.
Most of the medicines were still administered intravenously, but some, like the one for leukemia, were crushed and dissolved in water with a thickener and given to me with a teaspoon, as with children when they learn to eat. I still could not bring my hand from the glass to my mouth. Furthermore, the tremors would have caused most of the thickened liquid to end up everywhere except in my mouth.
The bed with side rails
I was lying on my back facing up; I saw the white ceiling with a window to my left that allowed me to see what was happening outside. But to be honest, I did not have a great interest in seeing what was happening outside; my thoughts were clouded. It seemed to me that I was on an island where thoughts did not exist, fear did not exist, pain was not felt, and time did not matter. I struggled to distinguish day from night and personally did not care to be aware of it.
One thing that disturbed me, however, was the bed rails, which I could not grab to turn onto my side. After many hours spent supine, where the only movements I could perform were moving my head to the right and left and my left arm, which I could drag across the sheets to the outer edge of the bed. Yes, on March 7 (described in the inpatient diary), I had begun to move my left hand.
This had already been a first sign of progress; then, as the days and weeks passed, I managed to move my arm as well.
The fact that I could move my arm gave me the conviction that I could grab the bed rail and, by pulling it toward myself, I could rotate my body and turn onto my side.
It was a pure illusion; I moved my arm, yes, but it was not yet able to overcome the force of gravity, let alone move a body—even though I had lost a lot of weight, I still weighed 52 kg.
I remember that the buttons to control the bed were on the rail, but even in that case, there was no question of being able to raise or lower the head of the bed; the rail was too far away, and furthermore, the tremor did not allow me to reach and maintain pressure on the button.
These difficulties demoralized me greatly; I was beginning to understand what kind of situation I had gotten myself into, and slowly I realized that I would not be able to return to the person I was before.
In fact, the nurses wrote in the inpatient diary:
“It is the first day I have cared for you and I am happy to see the good steps forward you have made; you are quite demoralized because you are beginning to realize the situation, but you continue to take small steps toward recovery.”
The transfer from bed to armchair
My body had not gotten up independently from the bed since January 12, 2021.
I was lifted thanks to the hoist, which allowed the nurses not to break their backs, even though my weight had decreased by over 25 kg. The sensation the hoist gave was not pleasant; I was in a bag suspended in mid-air and saw very little of what was happening to me, but that was how it was and I had to adapt.
Slowly, as the weeks passed, I began to have a little strength in my left hand, and then one of the nurses said to me: “Today we are trying a new technique; you will have to hug me intensely as if you were hugging your wife.” Initially, I did not understand, but then he approached and leaned down toward me, took my hands, and placed them around his neck. At 그 point he said to me: “Now hold your hands, I’ll do the rest; we’ll stand up and then rotate toward the armchair.” I was bewildered because the only muscles I could move were those of my left hand, and even with that, it’s not like I had monstrous strength. He said to me: “One, two, three, and go!”. He stood up with me hugged around his neck, turned, and gently placed me in the armchair.
His response was: “See, we made it!”.
For me, that day was a success; I no longer needed… or almost no longer needed that hoist.
In the following days, we still tried to use that technique to move me from the bed to the armchair and vice versa, but it did not always work; many nurses were afraid to lift me like that, others did not have the strength and therefore preferred to be in pairs, but in that case, the synchronization of movements in lifting me was difficult.
As time went by, however, I too learned to know my nurses and knew how to adapt to their lifting techniques. The important thing was to be able to get up for a few hours from that cursed bed and look around a bit.
On March 16, 2021, the nurses wrote to me: “Today you were in the armchair for more than 5 hours; for the whole day you did not need the ventilator, a high flow of air and oxygen was sufficient.”
Surely a success, a first step toward recovery? I had been in a hospital bed since January 12, and this was beginning to worry me. Furthermore, I knew that my parents were at the Clinica Luganese Moncucco; both were in intensive care and this worried me. I knew that my father had little chance of recovering, but for my mother, the doctors were optimistic; they had even extubated her.
This information of mine, however, dated back to mid-January and although I had a strange perception of time, probably due to the medications I was receiving, I began to think more and more about them and how they might be. As the days passed, this concern turned more and more into fear.
I asked the nurses if they had news of my parents, but they politely told me they were at the Cardiocentro and had no information about them. In hindsight, however, I came to know that everyone except me knew, but given my state, they did not want to burden me with further pain.
I learned of my parents’ death toward the end of March 2021; I learned it from my wife.
I suspected it because as soon as I brought up that subject or asked about them, everyone tried to change the subject or left.
I do not know if it was thanks to the medications or the weakness of the body, but I must say that at that moment the pain and regret were not so intense; finally I knew, but I still did not realize it.
The real pain and the sense of loss, however, were not long in coming; in the following months, when I had returned home, I began to realize what had happened to me and the loss. Before all this, my mother and father would visit us weekly; on those occasions, they would arrive with a crate of delicacies my mother had cooked and a few bottles of wine to enjoy the excellent food. They would stay for lunch until late afternoon before saying goodbye and returning to their nest, a small but nice apartment in Vacallo.
None of this would happen anymore; I would no longer see their faces, their behaviors when they argued because they disagreed on something—most of the time it was trifles or misunderstandings.
All this would no longer be, and will never be again!
The alarms – the blood pressure cuff and the oximetry sensor
I was awake; I saw and understood what was happening around me.
To be honest, I cannot say I was completely conscious; I still felt as if I were in a protective bubble. I felt no pain, and as soon as I said I felt pain or discomfort, they immediately rushed to me to try to solve the problem. I was a bit like the mascot of the intensive care unit; I had been with them for months now.
I remember I had the tracheostomy and they often had to suction me to clear the mucus and allow me to breathe better. As soon as I heard the gurgling through the tracheostomy, I would raise the palm of my left hand and they would immediately arrive to suction me; it had become almost a code signal that they understood instantly.
Despite this, I still had a lot of medical devices connected to my body and these were quite annoying.
I remember even today that the two most annoying devices were the blood pressure cuff and the oximetry sensor. During the day, it was bearable, but at night it was very irritating; every hour (I presume) it would start to inflate, and just as I was falling asleep, that gadget would compress my arm and wake me up.
If things went well, it was just the compression on the arm, but often some alarm would start ringing and shortly after the nurses would arrive. Among themselves they would say: “give him xx of NORA”; I always wondered what this NORA could be that was administered to me every time the alarm bell started ringing.
Now, after some questions and research, I have understood that NORA is the abbreviation for noradrenaline, a medication that primarily has these characteristics:
The effects of noradrenaline are mainly concentrated at the cardiovascular level.
Well known is its ability to increase heart rate and contractility, raising blood pressure through vasoconstriction.
In any case, that cuff that inflated regularly every hour, besides annoying me, allowed me to calculate how much time was left until morning.
Another device, not invasive at all but which annoyed me greatly, was the oximetry sensor.
It was attached to my finger 24 hours a day. My finger always felt sweaty, as if the skin could not breathe, so from time to time I would try to move it with the fingers that remained free, but as soon as I did, the alarm would start ringing. The same thing happened at night; if I happened to move my hand or fingers, the sensor would come off, causing me to wake up suddenly because of the alarm.
There were nurses who did not worry and as soon as the alarm rang they would arrive and check if the sensor was in its place, but there were also nurses who, after the first alarm, would take adhesive tape (or an adhesive bandage) and fix the sensor to me so it would not come off.
This bandage was very annoying; furthermore, it irritated the skin, as it remained stuck to my finger for many hours and in some cases even for an entire day.
But toward the end of my stay in intensive care, at least the blood pressure cuff was removed during the night. Much more comfortable, but there was a downside: I no longer had a way to determine what point of the night I was at. Now the only method was to look out the window and see the dawn beginning to illuminate my room… even if the view was not much.

For now, that is all I remember; as soon as other memories surface, I will record them on this page.
Goodbye!
Note: the report has been intentionally anonymized by the undersigned by removing the names of the physicians
Lugano, April 2, 2021/sc
INTERNAL TRANSFER LETTER
| Achermann Mirko, Via Contrada San Marco 31a, Agno – 05/04/1967 |
Dear Colleague,
we hereby inform you regarding the above-named patient who was hospitalized in our intensive care unit from 2021-01-31 to 2021-03-25.
Diagnosis:
- Severe ARDS due to bilateral SARS-CoV-2 pneumonia, N501Y variant (first diagnosis 2021-01-07):
- Veno-venous Extra Corporeal Membrane Oxygenation (ECMO) from 2021-01-31 to 2021-02-18; Prone-supine positioning cycles from 2021-02-20 to 2021-02-22;
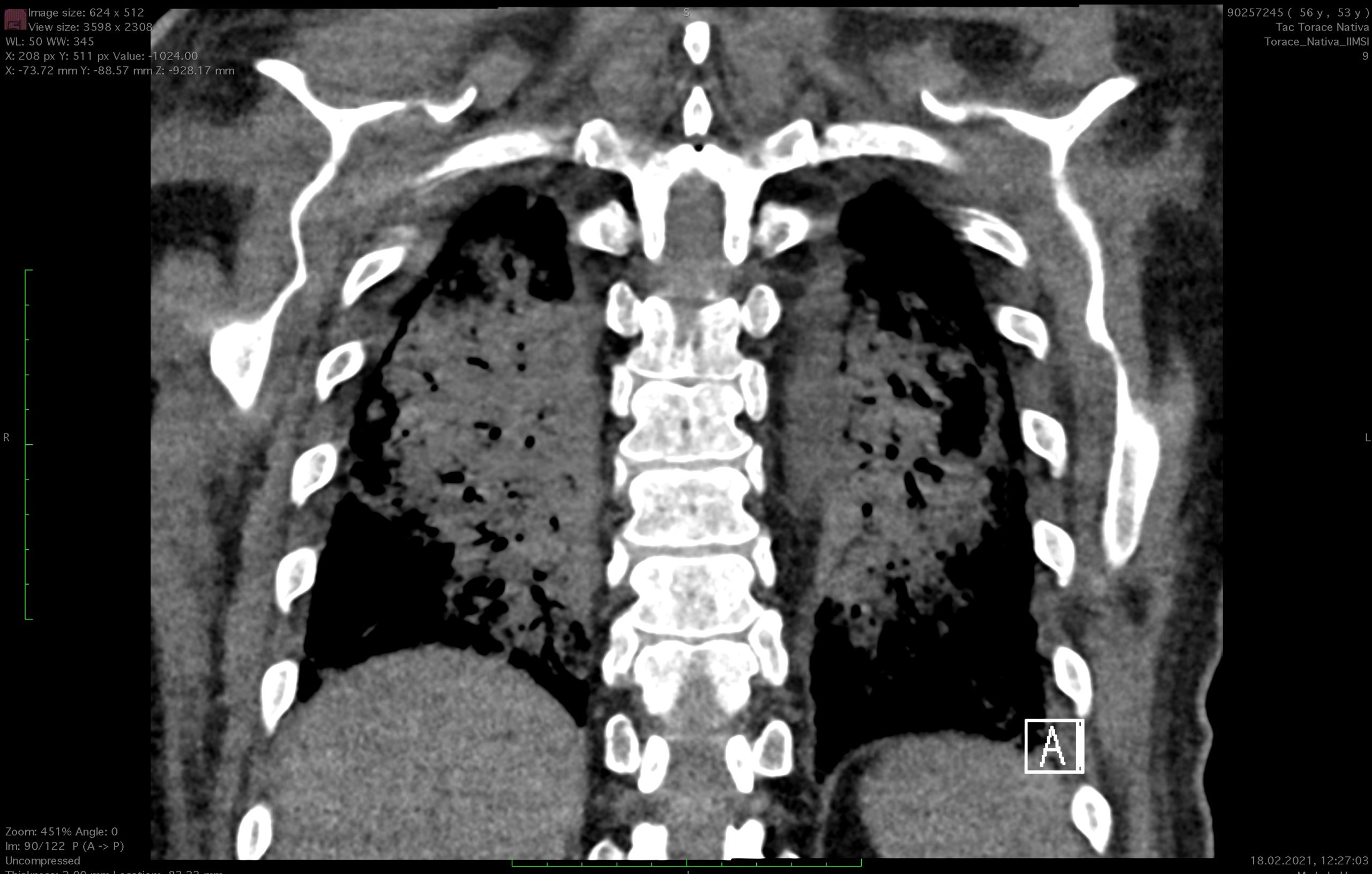
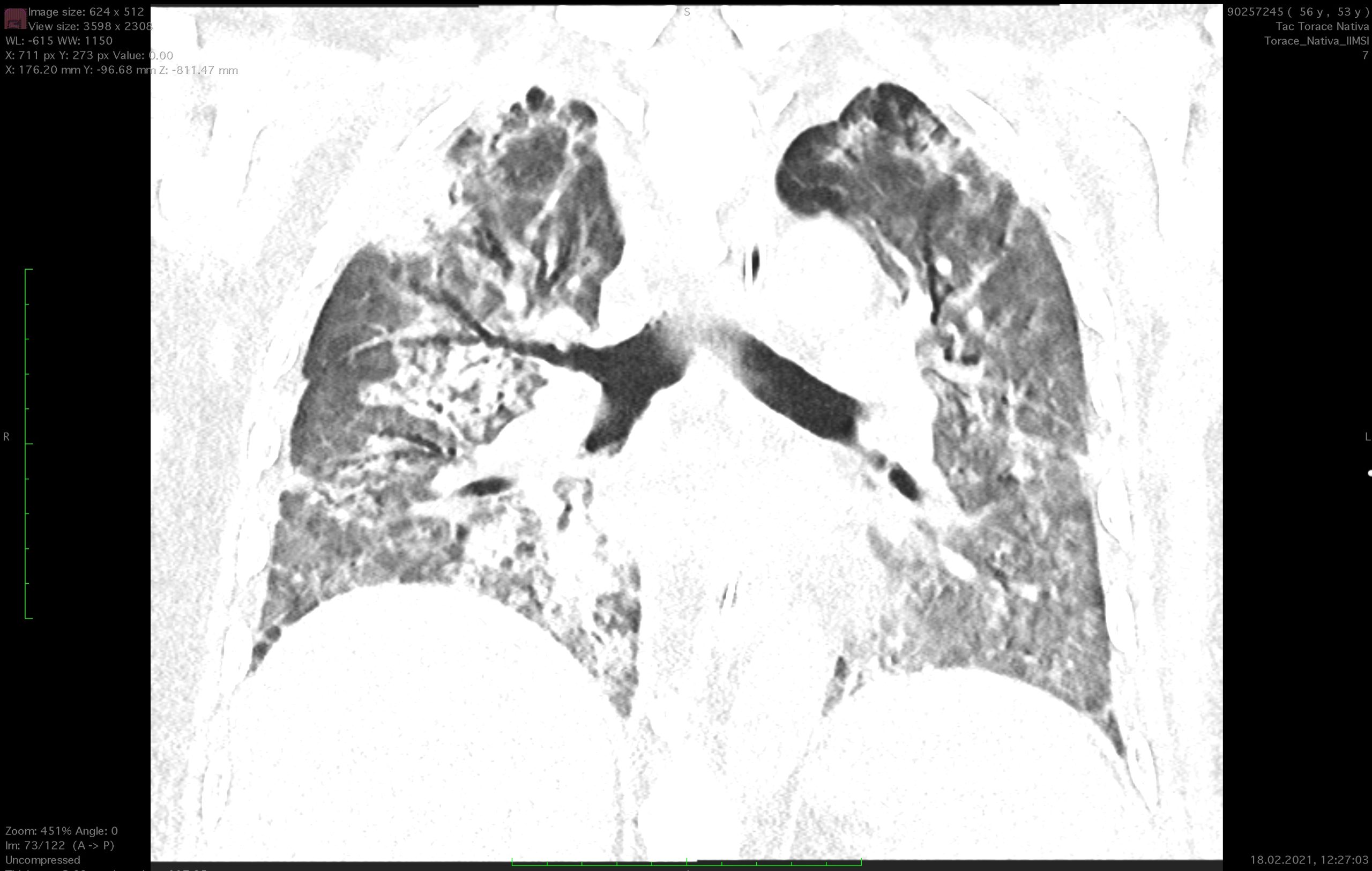
- Chest CT (Clinica Moncucco, 2021-01-23): diffuse bilateral infiltration progressing compared to the examination on 2021-01-13, no signs of pulmonary embolism.
- Non-contrast chest CT (2021-02-08): appearance of parenchymal consolidations with bronchiectatic alterations in the lower lobes, with suspicion of SOP (severe organizing pneumonia). In the remaining parenchyma, a lower intensity of ground-glass opacities present in previous checks on 2021-01-23 is observed.

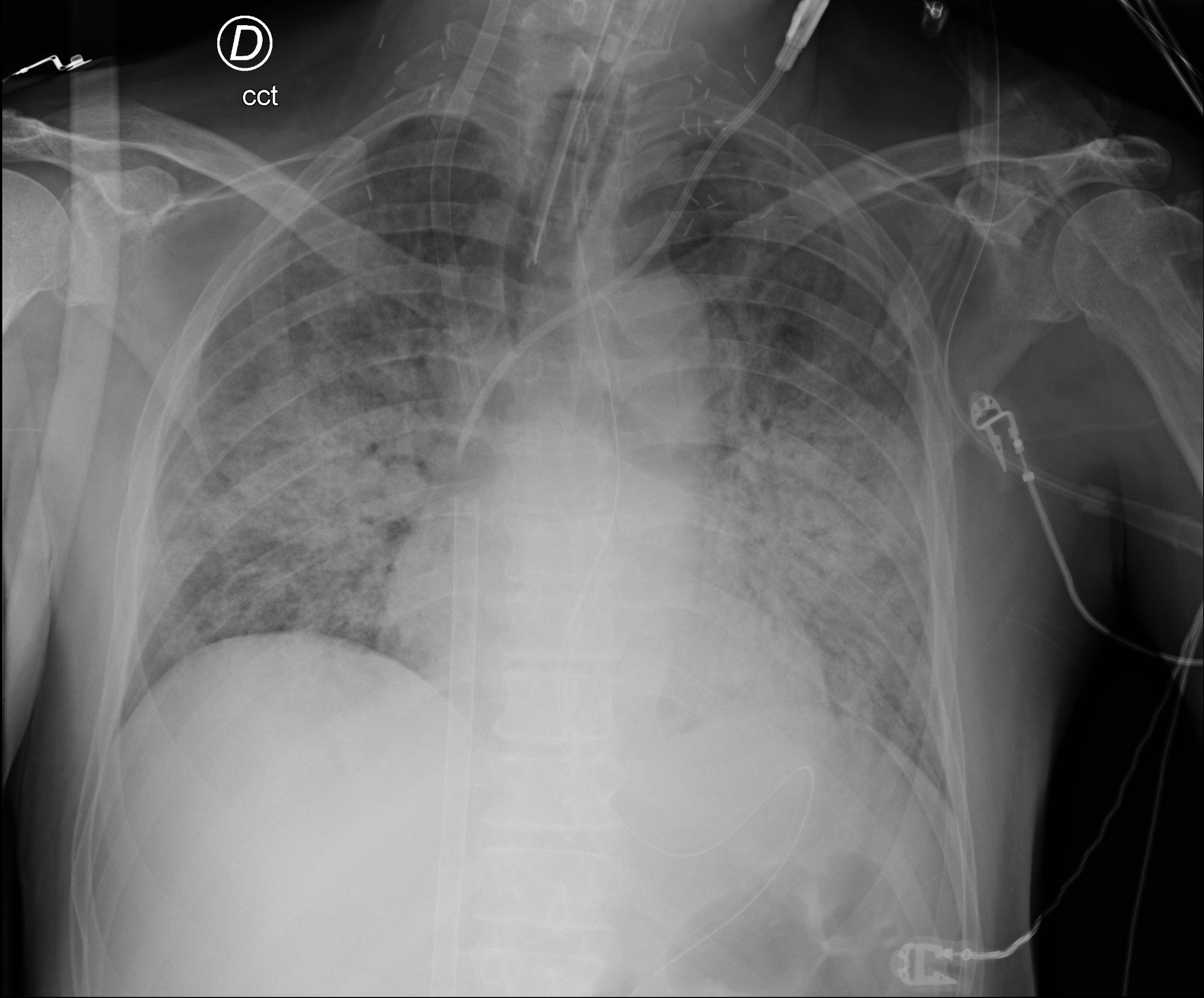
X-ray taken on 2021-02-01 at 00:14:56 upon my admission to the intensive care unit of Cardiocentro Ticino - Non-contrast chest CT (2021-02-18): at the parenchymal level, larger ground-glass areas and increased bilateral consolidation areas in the posterior segments of the upper and lower lobes. Aspiration phenomena from the tracheostomy.



- Thoraco-abdominal CT (2021-03-01): improvement of the pulmonary picture compared to the previous check where small bilateral peripheral infiltrates remain. Diffuse altered attenuation of the lung parenchyma suggestive of likely small airway disease.
- Non-contrast chest CT (2021-03-15): unchanged picture compared to the previous check on (2021-03-01) with persistence of small peripheral infiltrates bilaterally. Diffuse altered parenchymal attenuation suggestive of likely small airway disease.
- SARS-CoV-2
- Nasopharyngeal swab PCR (2021-02-01): positive; serum IgM negative / serum IgG positive (2021-02-10); N501Y mutation (2021-02-01): positive
- BAL PCR (2021-02-09, 2021-02-11): negative
- Stool PCR (2021-02-14): negative
- Actemra on 2021-01-16 (Clinica Moncucco)
- Dexamethasone 6 mg from 01-22 to 2021-01-31 (Clinica Moncucco)
- Solu-Medrol 80 mg from 2021-01-31 progressively tapered until 2021-02-23; Immunomodulation with Spironolactone and Azithromycin from 2021-02-09 to 2021-02-19
- Corticosteroid boost with Solu-Medrol 1 g/day (2021-02-24 to 26), 500 mg/day (2021-02-27 to 2021-03-01)
- Solu-Medrol 50 mg/day (from 2021-03-02)
- Transthoracic echocardiography (2021-03-10): Left ventricular size within normal limits. Preserved global systolic function (EF 55-60%). Left atrium of normal size. Tricuspid aortic valve, functioning normally. Minimal mitral regurgitation. Normal size and kinetics of the right ventricular cavity. Inferior vena cava not dilated, normally collapsing. Normal size of the aortic bulb (38 mm) and proximal ascending aorta (35 mm). Absence of pericardial effusion.
- In multifactorial global respiratory failure in the context of Ad1, ventilator-associated pneumonia, and intensive care unit myopathy:
- Placement of percutaneous tracheostomy on 2021-02-11
- Tracheostomy revision on 2021-02-12 and 2021-02-13; Bronchoscopy on 2021-02-13 and 2021-02-16
- Invasive ventilatory support from 2021-01-31 to 2021-03-23
- Klebsiella pneumoniae bacteremia on ventilator-associated pneumonia (VAP):
- Antibiotic therapy: Piperacillin-Tazobactam from 01-23 to 01-31 (Clinica Moncucco); Meropenem from 02-01 to 2021-02-10, Ceftriaxone from 02-10 to 02-14. 2021.
- Ventilator-associated pneumonia (VAP) from Enterococcus faecalis (bronchoalveolar lavage (2021-02-11):
- Cefepime from 2021-02-15 to 2021-02-20.
- Enterococcus faecium bacteremia of undetermined origin:
- Vancomycin from 2021-02-15 to 2021-02-22; Linezolid from 2021-02-23 to 2021-03-04.
- Febrile state of undetermined origin (FUO) DD Severe Organizing Pneumonia, drug-induced (antihistamine, neuroleptics), CML reactivation unlikely, rebound on steroid therapy reduction
- Acquired immunosuppression on high-dose steroid therapy:
- Prophylactic Meropenem therapy from 02-20 to 03-02, Co-trimoxazole therapy 3/week from 2021-03-01.
- Coagulopathy of multifactorial origin with anemia and thrombocytopenia:
- Mechanical hemolytic component on ECMO or consumption coagulopathy on bleeding, initial DIC
- Platelet nadir at 70 G/l on 2020-02-13
- Administration of 20 units of erythrocyte concentrates, 3 units of platelets, 4 units of fresh frozen plasma
- Brain CT (2021-02-18): no hemorrhagic lesions or densitometric alterations observed. Bleeding from tracheotomy requiring surgical revision (2021-02-12 and 2021-02-13)
- Severe Intensive Care myopathy with initial neuropathic component:
- Favored by high-dose steroid therapy
- Electroneuromyography (2021-03-11): axonal degeneration of the peroneal nerve bilaterally without further evidence of neuropathies
- Concomitant severe protein-energy malnutrition (NRS 7).
- Hyperkinetic Intensive Care delirium
- Generalized myoclonus with saccadic/ocular flutter or opsoclonus-myoclonus:
- Suspected post-Covid myoclonus
- Neurological physical examination (Dr. Galati, 2021-03-23): alert, cooperative, hypotonic speech. Ocular motility with intrusive saccades. Diffuse myoclonus, predominantly action-related, mixed positive and negative in the face, trunk, and limbs (predominantly left upper limb). No facial muscle deficits. Preserved head flexion. Lifts shoulders bilaterally MS-, shoulder abduction M4- bilaterally, greater hyposthenia on the right. Diffusely M3 in the right limb; in the left limb diffusely M4-. In the lower limbs, hip flexion and leg extension bilaterally M4; Plegia of dorsal flexion of the left foot; M4 plantar flexion of the feet bilaterally. Finger-to-nose test on the left possible with telekinetic tremor. Not evaluable on the right and heel-to-shin not evaluable due to paresis. DTR: right triceps reflex elicitable; other reflexes absent. Babinski: bilateral flexion
- Brain MRI with contrast (2021-03-24); findings within normal limits. Clinical improvement with Keppra therapy.
- Severe mixed dysphagia favored by Intensive Care myopathy:
- Speech therapy consultation (2021-03-15): complete dysphagia for solids and liquids, coughing with loss of paratracheal secretions
- Speech therapy consultation (2021-03-16): swallowing still ineffective, presence of coughing with paratracheal secretion drainage
- Speech therapy consultation (2021-03-18): improvement in swallowing, occasional coughing upon administration of water
- Speech therapy consultation (2021-03-22): no dysphagia during swallowing tests with solids and liquids. A dysphagic blended diet with non-thickened liquids and crushed medications is initiated.
- Chronic Myeloid Leukemia in chronic phase:
- Diagnosis 2020-09-28
- Peripheral blood smear (09-23): Marked neutrophilia, numerous myeloid precursors observed up to rare circulating blasts. Basophilia and eosinophilia
- Bone marrow aspirate (2020-09-28): Bone marrow of increased cellularity, characterized by myeloid hyperplasia, associated eosinophilia and basophilia, without excess of blasts (2.8% of total cellularity) immunophenotype: CD34+ elements are equal to 0.6% of the total
- Bone marrow biopsy (2020-09-28): histological finding consistent with myeloproliferative neoplasm type chronic myeloid leukemia; CD34+ blast count less than 5% of cellularity
- Cytogenetics: 46, XY, t(9;22)(q34;q11.2)[23)
- Molecular biology: BCR/ABL1 b3a2 (p210) fusion transcript present
- Abdominal ultrasound: Liver with homogeneous echostructure, normal in size, limits, and margins. Spleen of increased size (15.5 cm) risk scores: Sokal low (0.7), Hasford low (728.54), EUTOS low risk (46).
- Ongoing hematological therapy: Imatinib 400 mg 1x/day since 2020-10-03. Suspended from 2021-01-31 to 2021-03-12 per hematological indication. Resumed on 2021-03-12
- Peripheral blood smear (2021-03-03): anemia with reticulocytosis, isolated dacryocytes observed, neutrophilia with rare myeloid precursors up to an isolated blast
- Peripheral blood smear (2021-03-15): neutrophilic leukocytosis, neutrophils with toxic signs, myeloid precursors observed up to an isolated circulating blast. Finding consistent with known CML and reactive state.

Secondary diagnoses:
- Allergic asthma
- Bilateral thoracic outlet syndrome:
- Neurological symptoms treated with resection of the first right rib via supraclavicular approach with neurolysis of the brachial plexus (2018-01-18)
- Neurological symptoms treated with resection of the first right rib via supraclavicular approach with neurolysis of the brachial plexus (2018-01-18)
- Left L5 lumboradicular syndrome:
- Results of left L5 periradicular infiltration (2020-02-10)
- Results of L5-S1 stabilization (Dr. med. Liverani, 2000)
- Results of L4-L5 stabilization for left L5-S1 radiculopathy, removal of L5-S1 osteosynthesis material, except for screw in S1 on the left (2009)
- Sigmoidectomy for diverticulitis (2005)
Complicanze:
Bleeding from percutaneous tracheostomy with surgical revision on 02-12 and 2021-02-13.
Cardiovascular risk factors:
none.
Anamnesis:
53-year-old patient known for the diagnoses listed in the margin.
Followed by the Onco-hematology service for a recently diagnosed Chronic Myeloid Leukemia.
On 2021-01-07, a diagnosis of SARS-CoV-2 infection was made via nasal swab, initially in the absence of symptoms.
In the following days, worsening dyspnea appeared, requiring hospitalization from 2021-01-12 at Clinica Moncucco in Lugano.
The patient remains in the Intensive Care Unit from January 12, 2021 to January 19, 2021 and receives cycles of non-invasive ventilation (NIV) and a single dose of Tocilizumab on January 16, 2021.
Initially transferred to Internal Medicine, he returned to Intensive Care for respiratory failure requiring orotracheal intubation from 01-22 to 01-29. 2021.
Concurrently with the worsening, Dexamethasone therapy was introduced from 2021-01-22 for a total of 10 days and, under suspicion of pulmonary superinfection, Piperacillin-tazobactam therapy until 2021-01-28.
He benefited from prone-supine positioning cycles and protective ventilation.
Given the apparently favorable course, the patient was extubated on 2021-01-29.
On January 31, colleagues observe a new deterioration in respiratory gas exchange requiring new orotracheal intubation.
Given the progressive global respiratory failure despite invasive ventilation, with respiratory acidosis and high ventilation pressures non-responsive to pronation maneuvers, the patient was transferred to our Institute on the same day for veno-venous ECMO placement.
Procedures:
- Veno-venous Extra Corporeal Membrane Oxygenation (ECMO) (right femoro-jugular) from 01-31 to 2021-02-18;
- Mechanical ventilation from 01-31 to 2021-03-23;
- Percutaneous tracheostomy on 2021-02-11, Prof. Dr. med. Tiziano Cassina: see report;
- Surgical tracheostomy revision (2021-02-12 and 2021-02-13);
- Bronchoscopy (2021-02-13, 2021-02-16, OCL Pulmonologist): see report;
- Chest CT (2021-02-08, 2021-02-18, 2021-03-15): see report;
- Brain CT (2021-02-18): see report;
- Transthoracic echocardiography (2021-03-10): see report;
- Thoraco-abdominal CT (2021-03-01): see report;
- Electroneuromyography (2021-03-11): see report;
- Antibiotic therapy:
- Meropenem (2021-02-01 to 2021-02-10)
- Ceftriaxone (2021-02-10 to 2021-02-14)
- Cefepime (2021-02-15 to 2021-02-20)
- Vancomycin (2021-02-15 to 2021-02-22)
- Linezolid (2021-02-23 to 2021-03-04)
- Meropenem (2021-02-20 to 2021-03-02)
- Prophylactic Co-trimoxazole from 2021-03-01 to present (3 times per week);
- Blood cultures (2021-02-01, 12, 14, 19, 22, 27, 2021-03-01, 05, 07);
- Urine cultures (2021-02-01, 12, 2021-03-01, 05);
- Bronchoalveolar lavage (02-11, 02-22);
- Bronchial aspirate (2021-02-01, 04, 21, 28, 2021-03-05, 08);
- Urinary Legionella and Pneumococcus antigen (2021-02-01);
- Legionella PCR on BAL (02-11, 2021-02-22);
- Serum Aspergillus Galactomannan (02-20, 2021-03-05);
- Bronchial aspirate Aspergillus Galactomannan (2021-02-01, 11, 22, 2021-03-05);
- Serum Strongyloides (2021-02-20);
- Cytomegalovirus PCR (2021-02-04, 11, 22, 2021-03-02);
- Beta-glucan assay (2021-02-01, 20);
- Bronchial aspirate (2021-03-22);
- SARS-CoV-2 infection screening:
- Nasopharyngeal swab (2021-02-01)
- PCR on BAL (2021-02-09, 11)
- Stool PCR (2021-02-14)
- Serology (2021-02-10)
- Transfusion of 18 units of erythrocyte concentrates, 3 units of platelet concentrates, 4 units of fresh frozen plasma;
- Speech therapy consultation (2021-03-15, 16, 18, 22);
- Brain magnetic resonance imaging (2021-03-24): see report.
Course and discussion
Ad. 1-2:
Upon arrival, the patient was intubated, with inadequate respiratory exchanges in respiratory acidosis and severe hypoxemia.
Attempts to set up protective ventilation were ineffective, with plateau pressures (Pplat) remaining above 30 mmHg without any benefit to oxygenation.
After a collegial discussion, the decision was made for rapid placement of right femoro-jugular veno-venous Extra Corporeal Membrane Oxygenation (ECMO) on 2021-01-31.
The surgical procedure occurred without complications.
From an infectious standpoint (see Ad 3,4,5,6,7), considering the possibility of a bacterial pulmonary superinfection as a contributing cause of the new respiratory worsening, we broadened the antibiotic spectrum by initiating Meropenem.
In the context of “Unresolving ARDS,” we also began IV Methylprednisolone therapy at 80 mg/day.
Respiratory exchanges were entirely guaranteed by the ECMO in the first few days.
Initial assessments of pulmonary compliance performed on the sedated patient showed values below 20 ml/cmH2O.
After several attempts, we set up Duo-PAP ventilation, which allowed for maintaining excellent Pplat (around 20 cm H2O, progressively decreasing during the course) while ensuring the possibility of leaving the patient’s respiratory trigger, gradually reducing sedation.
With the strategies implemented, the patient shows minimal benefit in respiratory mechanics with improvement in pulmonary compliance around 27 ml/cmH2O, but gas exchange remains completely dependent on ECMO. On February 8, we perform a chest CT scan to rule out untreated pulmonary complications: The examination shows the appearance of parenchymal consolidations with bronchiectatic changes in the lower lobes, with suspected Severe Organizing Pneumonia.
The ground-glass opacities typical of SARS-CoV-2 infection were in regression.
In light of the radiological reports, we decided to initiate immunomodulation therapy with Azithromycin and Spironolactone from 02-09 to 02-19 in addition to the corticosteroid therapy.
Given the long duration of intubation, the lack of short-term prospects for extubation, and to reduce dead space and be able to progressively discontinue the patient’s sedation, we placed a percutaneous tracheotomy on 2021-02-11.
Although the procedure occurred without technical difficulties, we witnessed the appearance after a few hours of local bleeding, both external and internal (aspiration of abundant blood material from the trachea).
We performed two surgical revisions on 02-12 and subsequently on 02-13 without identifying a clear source of active bleeding.
During the course, bleeding remains present and diffuse, likely favored by the onset of concomitant ECMO-related coagulopathy (see Ad.7). We subject the patient to multiple bronchial toilettes to aspirate clots from the airways resulting from tracheal bleeding.
On 02-16, a thorough bronchoscopy performed by pulmonology colleagues from the Ospedale Civico di Lugano became necessary due to almost complete obstruction of the lower airways.
We subsequently witnessed a slow and progressive improvement in pulmonary compliance with an increase in ventilation volumes and improvement in respiratory exchanges, allowing for the progressive weaning of ECMO support.
On 02-18, we subjected the patient to a new chest CT showing a pulmonary picture substantially similar to the previous one.
Despite the slow radiological evolution, both oxygenation and ventilation were adequate and fully guaranteed by the patient with minimal ECMO support.
This allowed us to permanently remove the V-V ECMO on 02-18 without periprocedural complications.
With the subsequent discontinuation of the ECMO, we finally witnessed the complete resolution of the coagulopathy, and the tracheal bleeding rapidly and permanently self-limited without further obstructive episodes.
In the following hours, we maintained the patient on pressure-controlled ventilation interspersed with intervals of pressure support.
Ventilation volumes were adequate and respiratory exchanges satisfactory.
48 hours after the removal of the ECMO, although oxygenation remained at optimal levels, we witnessed a maladaptation of the patient to mechanical ventilation with progressive and severe hypercapnia, resulting in respiratory acidosis non-responsive to changes in the ventilatory setting. We therefore decided to perform pronation cycles from 2021-02-20 to 2021-02-23 with benefit to both carbon dioxide wash-out and respiratory mechanics, also thanks to better clearance of secretions with further clinical benefit.
Suspecting Severe Organizing Pneumonia not sufficiently improved with previous therapies, after a pulmonology consultation, we decided to undertake high-dose steroid therapy: we administered a boost of 1 g/day of Methylprednisolone from 2021-02-24 to 2021-02-26 (3 total doses), followed by 500 mg/day starting from 2021-02-27 until 2021-03-01.
The subsequent regimen from 03-02 is 0.75 mg/kg/day for 30 days (50 mg/day until 2021-04-01), followed by a further reduction to 0.50 mg/kg/day for another 30 days.
A new chest CT after the Methylprednisolone boost performed on 2021-03-01 showed a clear improvement in the pulmonary picture with signs of suspected small airway disease.
Although the first mobilizations to a chair were extremely difficult, with respiratory fatigue and complete dependence on the ventilator, as the days passed, the patient became increasingly autonomous and resistant to physical exertion.
The last follow-up chest CT on 03-15 shows a substantially stationary pulmonary picture.
Thanks to the therapies undertaken, we are witnessing a daily improvement in respiratory mechanics and exchanges.
We are progressively able to reduce respiratory support until maintaining the patient on spontaneous breathing.
The patient still benefits from CPAP cycles interspersed with high-flow ventilation.
Phonation attempts with a dedicated cannula are well tolerated, and we were able to permanently remove the percutaneous tracheostomy on 2021-03-23.
At the time of transfer, the patient is no longer dependent on daytime and/or nighttime oxygen therapy at rest.
As per agreements with Dr. …, the reference pulmonologist during the stay, the patient will be followed at the Hildebrand Clinic and must continue pulmonological follow-up.
Ad. 3-4-5-6-7:
Upon admission, the nasal swab was repeated, confirming SARS-CoV-2 infection, N501Y variant.
After discussion with infectious disease colleagues, the patient was not considered a candidate for further specialized therapies.
Suspecting a bacterial pulmonary superinfection as the cause of the patient’s new and rapid deterioration, we initiate therapy with Meropenem from January 31. The bronchial aspirate and blood cultures performed at admission will show the growth of Klebsiella pneumoniae, sensitive to the current therapy, but resistant to the recent antibiotic therapy with Piperacillin-tazobactam previously administered.
Urine culture, urinary antigens for Legionella and Pneumococcus, the search for Aspergillus galactomannan in the bronchial aspirate, and Beta-glucan performed on 01-31 were negative.
We performed another bronchial aspirate and serum CMV screening on 02-04, which were negative.
The inflammatory course is slowly favorable with a decrease in inflammatory parameters: we continued Meropenem therapy until 02-10 and, according to the antibiogram, concluded the antibiotic cycle with Ceftriaxone from 2021-02-10 to 2021-02-14.
Starting from 02-11, fever appeared along with a new rise in inflammatory parameters: suspecting an unresolved focus, we repeated blood cultures (2021-02-12 and 14) and urine cultures (2021-02-12) and performed a bronchoalveolar lavage with, in addition to general bacteriology, specific screening for Legionella and Aspergillus Galactomannan (2021-02-11).
We repeated CMV serology to exclude a possible reactivation, which was negative.
Antibiotic therapy was broadened by replacing Ceftriaxone with Cefepime from 02-15.
Culture tests showed the growth of Enterococcus faecalis in the BAL (2021-02-11), sensitive to the current therapy, and Enterococcus faecium in the blood cultures (2021-02-12), requiring the introduction of Vancomycin according to the antibiogram.
The rest of the cultures performed between 02-11 and 2021-02-14 were negative.
Ventilator-associated pneumonia from Enterococcus faecalis was treated with Cefepime until 2021-02-20.
Regarding the Enterococcus faecium bacteremia, we consider the lung as the possible starting focus, also in light of the CT images from 02-18 showing bilateral pulmonary consolidation areas.
Vancomycin therapy was discontinued on 02-22 in favor of Linezolid, an antibiotic with better penetration into lung tissue.
We continued with the prescribed therapy until 2021-03-04
Despite targeted therapies, the patient remained subfebrile with a stable inflammatory syndrome.
After the appearance of clear febrile spikes starting from 2021-02-19, considering the patient’s extreme immune fragility, we again repeated a broad panel of culture tests: serial blood cultures (2021-02-19, 22, 27), bronchial aspirate (2021-02-21), and BAL (2021-02-22, 28) with screening for Legionella and Aspergillus Galactomannan, CMV and Strongyloides serologies, and Beta-glucan assay.
We maintained antibiotic prophylaxis with Meropenem from 2021-02-20.
All tests performed were negative.
During the course, there was a slow decrease in inflammatory parameters, without ever reaching a clear normalization.
Meropenem therapy was discontinued on 2021-03-02.
Considering the high-dose steroid therapy ongoing for nearly two months and resulting in an effective state of immunosuppression, after an infectious disease consultation, we decided to maintain prophylaxis with thrice-weekly Co-trimoxazole starting from 2021-03-01.
After a few days without febrile spikes, starting from 2021-03-01, the patient became subfebrile again.
The inflammatory parameters, which never fully dropped, remained stationary.
As a precaution, we again repeated culture tests: serial blood cultures (2021-03-01, 05, 07), urine cultures (2021-03-01, 05), bronchial aspirate (2021-03-05, 08), serum and bronchial aspirate screening for Aspergillus-Galactomannan (2021-03-05), and CMV screening.
Taking into account that respiratory exchanges were always adequate and the absence of hemodynamic changes that might lead us to suspect an imminent septic state, we decided not to start a new antibiotic therapy.
All culture tests performed were negative.
As a cause of the febrile and inflammatory state, given the absence of a clear infectious cause, a possible SOP, a pharmacological origin from the ongoing antihistamine and neuroleptic therapy (see Ad. 9-10), an inflammatory rebound upon reduction of steroid therapy, or a reactivation of the known CML (see 13) are possible. As the days passed, and with the concomitant reduction of sedative therapy, there was a spontaneous and gradual disappearance of the fever with slow and complete normalization of inflammatory indices.
We note the possibility of de-isolating the patient starting from 2021-02-15, considering the negative SARS-CoV-2 PCR on the nasal swab from 2021-02-09, on the BAL from 02-11, and on the stool from 2021-02-10, and the presence of adequate antibody coverage (negative IgG and positive IgM on 2021-02-10).
The last bronchial aspirate from 03-22 performed on an afebrile patient without inflammatory indices showed no bacterial growth.
Ad. 8:
With the start of ECMO, there was immediately a mechanical hemolytic component characterized by anemia and thrombocytopenia requiring targeted transfusion support. Anticoagulation was maintained with Liquemin with an APTT around 50 sec.
As the days passed, we witnessed the appearance of a coagulopathy with diffuse bleeding from the tracheotomy, oral and nasal mucosae, the appearance of spontaneous hematomas, petechiae on the hands, and dark-colored urine.
Considering an extremely elevated D-dimer (maximum value on 2021-02-12 with 46.32 mg/l), although in the absence of clear fibrinogen consumption, we cannot exclude disseminated intravascular coagulopathy.
In the differential diagnosis, consumption coagulopathy from persistent bleeding or ECMO-induced coagulopathy are possible.
The peripheral blood smear excluded thrombotic microangiopathy.
Although there were no clear focal deficits, concurrently with the chest CT on 2021-02-18, we performed a brain CT which excluded intracranial bleeding.
With the discontinuation of ECMO support, the bleeding stopped spontaneously within a few hours.
During the course, we did not witness hemorrhagic recurrences and continued anticoagulation with Liquemin in the therapeutic range.
Given the subsequent sharp drop in D-dimers and the inflammatory syndrome, we continued with prophylaxis only starting from 2021-03-17.
Hemoglobin and platelets remained stable with a discharge value of 92 g/dl and 153 G/l, respectively.
Ad. 9-10-11:
Upon admission to Intensive Care, multimodal sedation was necessary to ensure adequate adaptation to the ventilator.
Daily neurological assessments allowed for excluding the appearance of focal deficits and ensuring good patient comfort.
Once the acute phase was passed and ECMO support removed, we progressively reduced sedation.
Hyperkinetic delirium with agitation, anxiety, respiratory maladaptation, and severe nighttime and daytime insomnia became immediately evident.
We progressively titrated multimodal neuroleptic and sedative therapy (benzodiazepines, neuroleptics, antihistamine); during the first few days, the patient benefited from sedation first with Propofol and then with nighttime Dexdor.
With the strategies implemented, there was a slow and progressive clinical improvement: the patient resumed regular day-night cycles and was well-cooperative and proactive. The prescribed therapy was progressively reduced and adapted to the patient’s needs.
Severe Intensive Care myopathy developed rapidly due to forced bed rest for ECMO, numerous infectious complications, and catabolic high-dose steroid therapy.
Upon discontinuation of ECMO, the patient appeared cachectic with severe muscle atrophy resulting in a state of tetraplegia.
Thanks to rapidly initiated physiotherapy, muscle tone was partially recovered: autonomous mobilization of proximal muscles and decent trunk control became possible, while peripheral and fine motor skills have not yet been recovered.
Transfer to a chair with assistance is possible.
Respiratory muscles also progressively regained strength, such that it was possible to remove the tracheostomy on 2021-03-24.
We are continuing with respiratory physiotherapy with benefit.
An electroneuromyography performed on 2021-03-11 for prognostic purposes showed only an initial peripheral-distal neuropathic component in the peroneal nerves bilaterally; the rest of the picture remains compatible with myopathy secondary to the critical state and prolonged corticosteroid therapy.
With the resumption of autonomous mobilization, diffuse myoclonus/opisthotonos became evident, especially in the facial muscles, tongue, and upper limbs.
After a neurological consultation, we initiated Keppra therapy and performed a brain MRI which excluded a post-anoxic or ischemic form.
A post-infectious form is possible; given the current state of immunosuppression and the improvement with the initiated therapy, we prefer to abstain from performing a lumbar puncture to exclude paraneoplastic or autoimmune forms.
The tremors are progressively improving with the prescribed therapy; an intentional component persists.
We leave it to colleagues at Hildebrand to evaluate the optimization of therapy and any further investigations.
Ad. 12:
From admission, the patient benefited from enteral nutrition at a caloric target via a nasogastric tube (NGT).
Hypophosphatemia present in the first days of refeeding was rapidly corrected.
The abdomen was always calm with bowel movements of formed stools.
Given the evident multifactorial malnutrition and severe Intensive Care myopathy, and aware of the high risk of dysphagia, we subjected the patient to a speech therapy consultation on 2021-03-15, which confirmed the clinical suspicion.
Thanks to continued physiotherapy and the performance of targeted speech therapy exercises, the dysphagia is progressively improving, and we can resume a blended diet. After the removal of the tracheotomy, good swallowing persists without signs of dysphagia, allowing for the removal of the NGT and the resumption of a normal diet.
Ad. 13:
The patient is known for Chronic Myeloid Leukemia treated with Imatinib.
Upon admission, considering the risk of pulmonary toxicity from the therapy, in agreement with the treating hematologist, we decided to suspend the chemotherapy agent.
The recurrence of an inflammatory syndrome and febrile spikes from 2021-03-01 in the absence of a clear infectious focus raised clinical suspicion of disease reactivation.
On hematological advice, we performed a peripheral blood smear which excluded the presence of circulating blasts.
Considering the good clinical stability and the progressively favorable course, we decided to resume Imatinib therapy starting from 2021-03-12 in agreement with the treating hematologist.
On 2021-03-25, we are transferring Mr. Achermann to the Ward in anticipation of his transfer to the Hildebrand Clinic.
Plan:
- Arrange transfer to Hildebrand Clinic in one week according to availability;
- Continue from 2021-04-01 with Prednisone 30 mg/day, subsequent tapering to be discussed with the treating pulmonologist Dr. …;
- Continue with prophylactic Bactrim until pulmonological re-evaluation;
- Continue with the prescribed neurological therapy of Keppra, re-evaluate with colleagues at Hildebrand for therapy modifications or any further investigations according to the evolution of the tremors;
- Continue with respiratory and mobilization physiotherapy;
- As requested by Dr. …, the treating hematologist, arrange for blood BCR/ABL1 assay for monitoring the known CML.
Therapy at discharge:
See computerized chart Whale.
We remain at your disposal and send cordial regards.
Prof. Dr. med. …
Dr. med. …
Dr. med. …
Good morning, Mr. Achermann,
I am Maura; I will be looking after you again this morning.
You are awake today and I am finally able to communicate with you; you are nodding your head, attempting to speak (though your voice cannot come out until you are off the ventilator), and you smiled at me.
This morning I gave you your “beauty treatments” and after performing motor physiotherapy in bed, the physiotherapist and I helped you sit in an armchair.
We used a lift, as you are still weak, but this morning I saw you move your left hand.
I am pleased to see your progress.
In a little while, I will put you back to bed and let you rest; being seated in the armchair is a great effort for you at the moment.
Stay strong!
Maura
Good morning, Mr. Mirko, I am Stefania, a nurse.
Since the day of your admission, I have not been directly caring for you, but I have been following your progress nonetheless.
The ECMO, the machine that supports your lungs, is still necessary.
In recent days, you underwent a tracheostomy—a hole in your neck that allows you to breathe; the tube in your mouth that was causing you so much discomfort has been removed.
The medications that keep you sedated are still necessary, but when I entered the room, I had the impression that you could hear me: you move your eyelids when I speak to you, but you do not open your eyes.
Your forehead is also a bit “furrowed”… perhaps you can hear me!
I explained to you that you cannot move your arms and legs due to the number of days you have been immobile in bed.
I had to remove mucus from the hole in your neck; you have the strength to cough, but you are unable to expel the secretions.
The attending physician is always in contact with your wife and keeps her updated on the situation.
I am now returning to the room to administer your 6:00 PM medication.
I hope to see you more awake tomorrow morning.
I will say goodbye for now.
Stefania